EVALUATION AND TREATMENT
Physical therapy
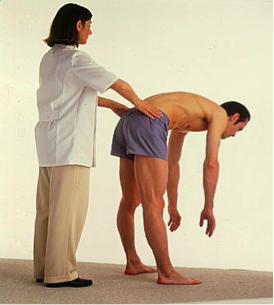
evaluation, after taking a thorough history of the injury, starts with the
observation of the patient’s gait and transition from one position to another.
It continues with the assessment of the lumbar range of motion and the effects
of the repeated movements on the location of radicular (going down the leg)
symptoms.

The assessment of the
pelvic alignment is necessary and the differentiation is made between a shift
which is usually a sign of a herniated disk (the patient’s upper body is
shifted away from the injured side, thus producing a pelvic shift towards the
side of the herniated disk) and pelvic misalignment which is usually a sign of
a sacroiliac joint problem. I have treated many patients who experience a
dramatic improvement of symptoms after the pelvis was re-aligned.
Major lower extremities
joints’ range of motion is assessed and followed by the strength testing of the
lower extremities and abdominals, including deep abdominal muscles that
stabilize the spine.
A thorough physical therapy
evaluation identifies the cause of the patient’s symptoms and sets up an
appropriate treatment plan.
If the symptoms were
created by a herniated disc the treatment is focused on the centralization of
the pain. This means that the primary goal of the treatment is to get rid of
the pain in the leg and centralize it in the lower back. After this is
achieved, next goal is to abolish the pain completely.
If the symptoms are caused
by mechanical low back problem (such as a sprain or an abnormal movement in one
or more spinal joints) or the sacroiliac joint problem, the treatment focuses
on manual therapy for restoration of normal joint mechanics, strength, and
position sense of lumbar-pelvic area. Core stabilization program is always
included in the treatment, regardless of the cause.
Contrary to some opinions,
therapy should not be painful but should lessen the pain with every treatment.
Effective physical therapy should be based on manual therapy with a hands-on
approach to exercises performed by licensed therapists.

If unresolved fast, low
back problems become chronic and can be very frustrating for the patients and
health care providers. Patients with chronic low back pain or sciatica may
become very dependent on narcotic pain medications. However, if rehabilitated
timely and properly, low back pain patients recover fast and, with correct
postural and body mechanics education, become much more aware of potential
problems and learn to avoid new injuries.
Take a quiz and get a chance to win a tube of Biofreeze for
fast, drug-free pain relief!
1. True or False: Sciatica
is more prevalent in women 30 years and older.
2.
True or False: Sitting is great for
treatment of most herniated disks.
3. True or False: Primary
goal of the treatment is to get rid of the pain in the leg and centralize
it in the lower back.
4. True or False: Physical
Therapy should be painful.
You can post your answers
as comments or you can email them to me at michaelpt.freemotion@gmail.com.
First 20 people to respond will be entered to win (3 tubes of Biofreeze will be
given away!)
Stay healthy and take care
of your back!
Michael Sheynin, PT, Co-owner of Free Motion Rehab Center



{kind=link}